
Health and social care work is intimate. Care workers help people wash and dress, eat and drink, manage medication, navigate end-of-life decisions, hold on to identity through dementia. The relationship between a care worker and the person they support is closer than almost any other professional relationship in modern Britain. That intimacy is exactly why equality and diversity matter here: when you're caring for someone day in and day out, every assumption you make about who they are, what they value and what they need is consequential.
This guide is for everyone working in or training for health and social care in the UK — health and care support workers, nurses, registered managers, social workers, allied health professionals. It explains what equality and diversity mean in a care context, the legal and regulatory framework that applies, what good person-centred care looks like, and the everyday situations where getting equality and diversity right (or wrong) makes a real difference to the people being supported.
What equality and diversity mean in a care setting
In a care setting, equality means giving everyone access to care that meets their needs, on the same basis as anyone else. Diversity means recognising that the people receiving care are individuals with their own backgrounds, beliefs, identities and preferences, and adjusting practice accordingly. The two work as a unit: a care service that treats everyone the same isn't being equal, it's being uniform, and the people who don't fit the default end up getting worse care.
This isn't an abstract principle. It's about whether the woman on the ward who only speaks Gujarati can actually communicate her pain levels, whether the resident who is gay feels able to display photos of his late partner, whether the person with learning disabilities is consulted about her own care plan rather than spoken about over her head, whether the patient who is fasting for Ramadan has his medication schedule adjusted to fit.
A foundational point in care: equality of treatment does not mean identical treatment. The Care Quality Commission and Skills for Care both make this clear. The person-centred approach that runs through modern UK care practice is built on the idea that fair care attends to the individual person — their needs, their preferences, their identity — rather than applying the same approach to everyone regardless.
The Care Certificate Standard 4
The Care Certificate is the induction framework for healthcare support workers and adult social care workers in England, developed by Skills for Care, Skills for Health and Health Education England. It sets out the minimum knowledge, skills and behaviours expected of new staff in care roles.
Standard 4 — Equality, Diversity, Inclusion and Human Rights — is one of the 15 core standards. It has three learning outcomes:
4.1 Understand the importance of equality and inclusion
This covers what equality, diversity, inclusion and discrimination mean in practical terms; the ways discrimination can occur deliberately or inadvertently in care work; and how inclusive practices reduce the likelihood of discrimination.
4.2 Work in an inclusive way
This covers identifying which legislation and codes of practice apply to the worker's own role; interacting with individuals in ways that respect their beliefs, culture, values and preferences; and challenging discrimination when it's encountered.
4.3 Access information, advice and support about diversity, equality and inclusion
This covers knowing where to get further information, advice and support; how and when to access it; and who to ask.
Each learning outcome breaks down into assessment criteria that the worker must demonstrate during their induction period. The Care Quality Commission expects providers to evidence Care Certificate completion as part of the induction of new staff.
A note for vocational learners: Standard 4 isn't a one-off ticked at induction and forgotten. The principles run through every other standard — particularly Standard 5 (person-centred care), Standard 6 (communication), Standard 7 (privacy and dignity), and Standard 10 (safeguarding adults). Equality and diversity in care are continuous practice, not a discrete topic.
The legal framework
Care providers in the UK operate under several overlapping legal frameworks. The most important are these.
The Equality Act 2010 prohibits discrimination on the basis of the nine protected characteristics — age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sex, and sexual orientation. Care providers are bound by these protections both as employers (in how they treat staff) and as service providers (in how they treat the people they care for). The duty to make reasonable adjustments applies — physical environment, communication formats, care plan design, all need to be adjusted where reasonable for disabled people. For NHS bodies and local authority commissioners, the Public Sector Equality Duty applies on top of the general prohibition on discrimination.
The Care Act 2014 sets out the legal duties of local authorities in adult social care. It includes a 'wellbeing principle' — promoting the wellbeing of the individual is the central purpose of the system — that explicitly covers control over day-to-day life, participation in work, education and recreation, social and economic wellbeing, and the suitability of living accommodation. The Act emphasises personalisation: care and support should be designed around the individual, not the service.
The Human Rights Act 1998 incorporates the European Convention on Human Rights into UK law. For care providers, the most relevant rights are Article 3 (prohibition of inhuman and degrading treatment), Article 8 (right to respect for private and family life), Article 9 (freedom of thought, conscience and religion), and Article 14 (prohibition of discrimination). Public bodies — including NHS trusts and local authorities — are directly bound; private and voluntary providers carrying out public functions on their behalf are bound when exercising those functions.
The Mental Capacity Act 2005 governs decision-making for people who lack capacity to make particular decisions for themselves. It is anchored in equality principles: the assumption of capacity, the right to make unwise decisions, the obligation to consider least restrictive options. Best interests decisions for people who lack capacity must take into account the person's past and present wishes, beliefs and values.
Care Quality Commission regulations — particularly the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014 — set out the standards CQC inspects against. Regulation 10 (dignity and respect) and Regulation 13 (safeguarding) both have explicit equality dimensions.
Person-centred care and equality
The phrase 'person-centred care' has become so common it can lose its meaning. In its substantive form it means three things:
The care is organised around the person as they actually are — their history, preferences, beliefs, identity, relationships, ways of communicating, things they enjoy, things they find distressing — rather than around the convenience of the service.
The person is a partner in their own care, consulted about decisions affecting them, with their views taken seriously even when they're unwise, unconventional or inconvenient.
The whole person matters, not just the medical or care need. Someone with dementia is still the person they always were; someone receiving palliative care is still living, not just dying; someone with a learning disability is still an adult.
Person-centred care done well is equality and diversity in practice. It can't work if the worker doesn't recognise the person's individuality, their cultural background, their faith, their relationships, their preferences. A care plan that records 'patient prefers cooked breakfast' but doesn't capture that the patient is a practising Muslim who doesn't eat pork is not really person-centred.
Examples in everyday care
The texture of equality and diversity in care is in concrete, ordinary moments.
Language and interpretation
Mrs Hussein, 78, on a hospital ward, speaks Urdu and limited English. She has been admitted with a urinary tract infection and her pain is being managed with paracetamol. The ward staff have been using her daughter as an interpreter, including for sensitive conversations about toileting and pain. The right approach is to use a professional interpreter — telephone, video, or in person — for clinical conversations. Family members shouldn't be used as default interpreters, particularly for intimate or sensitive matters.

Mealtimes and dietary observance
Mr Patel is a vegetarian for religious reasons; Mrs Cohen keeps kosher; Mr Khan is fasting for Ramadan and eats only between sunset and sunrise during that month. A care home that gets this right has a system for capturing these preferences at admission, communicating them across shifts, and adapting timings (medications, meals, drinks) accordingly. A care home that gets it wrong serves Mr Patel a meal with chicken stock, Mrs Cohen a milk-based dessert after meat, and asks Mr Khan to take his medication with food at 1pm during Ramadan.

Faith practice
Mrs Singh prays five times a day. The care plan accommodates this by ensuring she has access to a clean, quiet space (a screen around her bed if needed), her prayer mat is reachable, and her care isn't routinely scheduled during prayer times. Mr Williams is a regular churchgoer who can no longer attend services. A weekly visit from a hospital chaplain or local minister, organised through the chaplaincy service, is arranged.

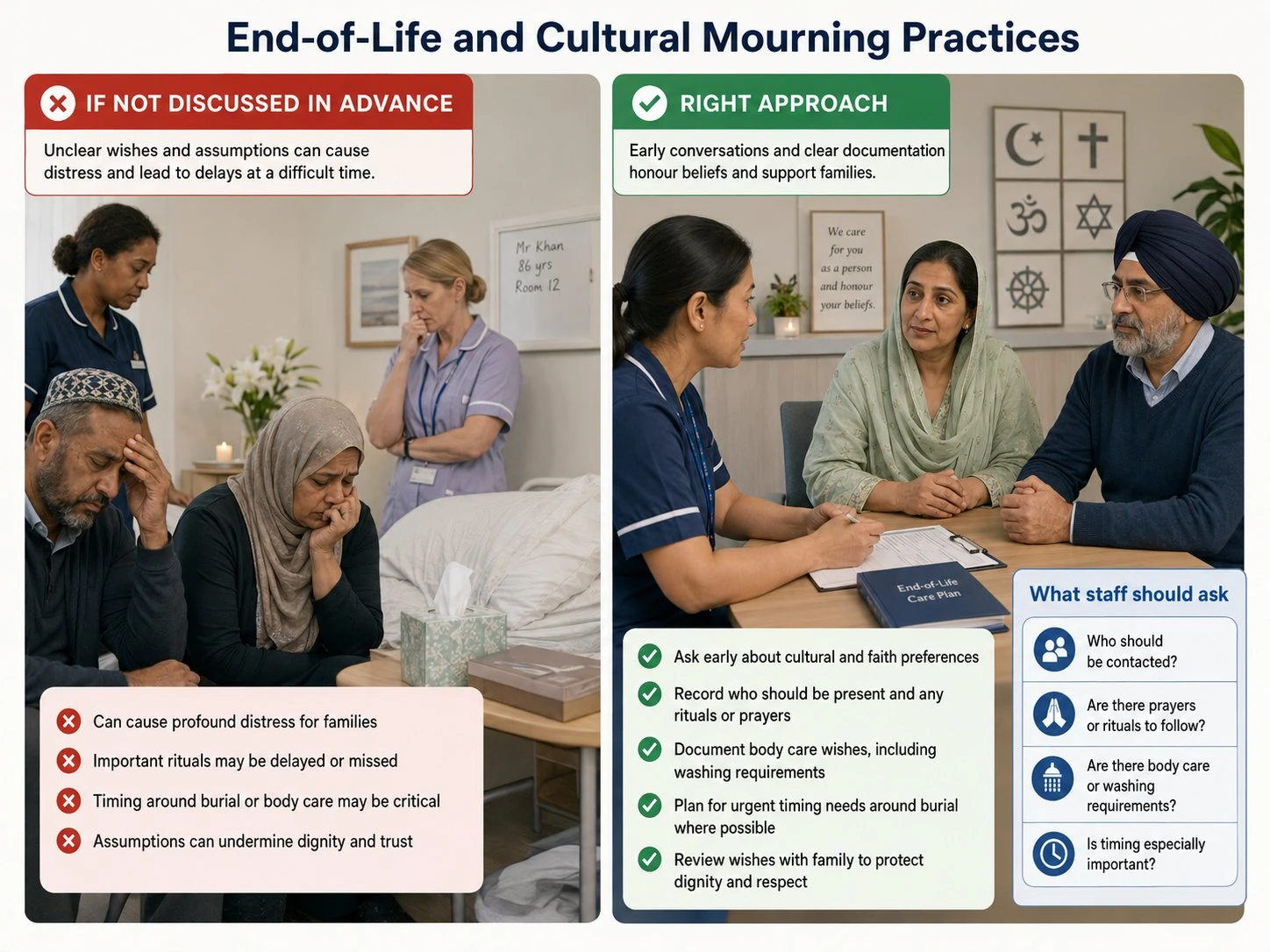
End-of-life and cultural mourning practices
Different cultures and faiths have very different practices around death — what should happen to the body, who should be present, what timing matters. Jewish tradition requires burial within 24 hours where possible; Muslim tradition similar; some traditions require specific people to wash the body; some require particular prayers or rituals. A hospice or care home that doesn't capture these expectations in advance can cause profound distress at the time of greatest vulnerability.
Family structure and LGBT+ residents
Mr Davies, 82, has lived with his partner Tom for 51 years. His care home asks about 'next of kin' on admission and assumes a heterosexual family structure. Mr Davies has to explain his relationship repeatedly to different staff. Tom is initially assumed by some staff to be a friend. The right approach is open intake questions that don't assume — 'who is important to you in your life and care?' — and active confirmation that same-sex partners are recognised as next of kin.

Age-related communication
Mr Roberts has dementia. He's also, before the dementia, was a chartered accountant and a competitive cyclist; he was articulate, sharp, and proud. A good care worker continues to address him as the adult he is, doesn't speak about him in his presence as if he isn't there, doesn't use 'elderspeak' (the slow, loud, sing-song register sometimes directed at older people), and finds ways to draw on the cognitive function he still has rather than treating him as cognitively absent.

Learning disability
Sarah, 34, has Down's syndrome and lives in supported accommodation. Decisions about her care are routinely taken in conversations between her staff team and her parents, with Sarah present but rarely consulted directly. The right approach, consistent with the Mental Capacity Act, is to consult Sarah herself, to use accessible information (easy-read documents, pictures, video where useful), to give her time to consider and respond, and to involve her parents as supporters rather than substitutes for her own decision-making.

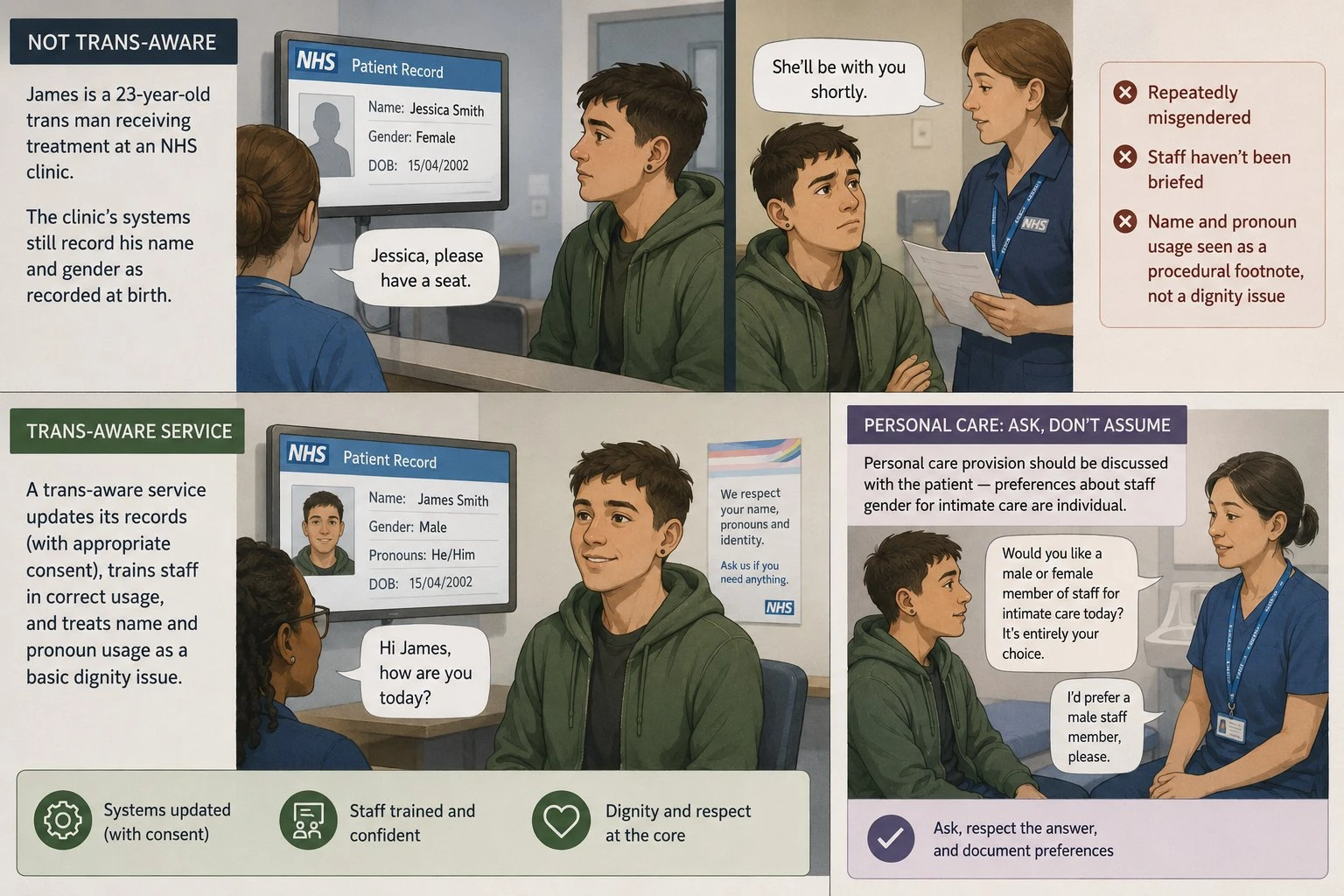
Gender identity and personal care
James is a 23-year-old trans man receiving treatment at an NHS clinic. The clinic's systems still record his name and gender as recorded at birth. He's repeatedly misgendered by staff who haven't been briefed. A trans-aware service updates its records (with appropriate consent), trains staff in correct usage, and treats name and pronoun usage as a basic dignity issue, not a procedural footnote. Personal care provision should be discussed with the patient — preferences about staff gender for intimate care are individual.
These examples are deliberately ordinary. They aren't dramatic; they're the texture of what care actually involves when it takes equality seriously.
Common scenarios and how to handle them
A few situations that come up regularly in UK care work.
A colleague says something discriminatory
A care worker hears another worker make a derogatory remark about a resident's faith. The right approach is to address it directly where safe to do so — 'we don't talk about residents like that here' — and to report it to a manager. Letting it pass condones it. Care workers have a duty to challenge discriminatory practice, captured in Standard 4 assessment criteria.
A resident or service user says something discriminatory
A resident with dementia uses a racial slur to a care worker of colour. The worker shouldn't take it personally and shouldn't escalate to confrontation, but should report it to the manager so that the team can respond consistently and so that the affected worker isn't left to absorb it. Repeated incidents may require a care plan adjustment, conversation with the resident's family, or — in extreme cases — review of the placement.
A family member directs care in ways the resident wouldn't choose
A family member instructs the care home not to allow the resident's same-sex partner to visit. The home's obligation is to the resident, not the family member; if the resident has capacity and wants the visits, they happen. If the resident lacks capacity, the question is what's in her best interests under the Mental Capacity Act, taking into account her past expressed wishes.
A resident's preferences conflict with another resident's needs
Mr A wants to watch loud TV; Mr B in the next room finds it distressing. The resolution isn't 'the loudest voice wins' but a negotiated compromise — timed quiet periods, headphones, room reallocation if needed.
Cultural practices that involve risk
Mrs B wishes to fast for religious reasons but is diabetic. The care team's role is to support her decision (she has the right to make decisions about her own body and faith), while making sure she has the information she needs and the medical support to do it safely.
Sources of further information
The most authoritative UK sources for equality and diversity in care work:
Skills for Care publishes the Care Certificate materials including the full Standard 4 workbook. The 15 standards are the foundation of induction in adult social care.
The Care Quality Commission inspects care providers against fundamental standards that include dignity and respect, person-centred care, and safeguarding.
The Equality and Human Rights Commission publishes statutory codes of practice on the Equality Act that apply to care providers as service providers and as employers.
ACAS is the key resource for equality and diversity in care employment — the employment side of running a care service.
The Health and Care Professions Council, the Nursing and Midwifery Council, and Social Work England each set professional standards that include equality and diversity elements for their registered professionals.
Frequently asked questions
What is equality and diversity in health and social care?
Equality is providing care on the same basis to everyone regardless of who they are; diversity is recognising that the people receiving care are individuals with their own backgrounds, beliefs, identities and preferences, and adjusting practice accordingly. Both are central to person-centred care.
What is Care Certificate Standard 4?
The Care Certificate Standard covering equality, diversity, inclusion and human rights. It has three learning outcomes — understanding the importance of equality and inclusion, working in an inclusive way, and accessing further information. It's part of the induction framework for healthcare support workers and adult social care workers in England.
What legislation applies to equality in care?
The Equality Act 2010 is the principal framework. Alongside it, the Care Act 2014 sets out duties around wellbeing and personalisation, the Human Rights Act 1998 provides additional protections, the Mental Capacity Act 2005 governs decision-making for people without capacity, and the Care Quality Commission regulations set the standards CQC inspects against.
What is person-centred care?
Care that is organised around the individual as they actually are — their history, preferences, beliefs, identity, relationships, ways of communicating — rather than around the convenience of the service. It treats the person as a partner in their own care and recognises the whole person, not just the medical or care need.
How do I challenge discriminatory practice in care?
Address it directly where safe — 'we don't talk about residents like that here'. Report it to a manager. Document what happened. Standard 4 of the Care Certificate includes the duty to challenge discrimination, and care workers' professional codes of conduct typically require it.
What is the Care Act 2014?
The Care Act 2014 sets out the legal framework for adult social care in England. Its 'wellbeing principle' makes promotion of individual wellbeing the central purpose of the system, and emphasises personalisation: care should be designed around the individual.
Do I need the Care Certificate?
If you're new to the adult social care sector or to a healthcare support worker role in the NHS in England, completion of the Care Certificate is expected as part of your induction. It's not a formal qualification in the regulated sense but it's the recognised standard for induction across the sector.
How does the Equality Act 2010 apply in care?
Care providers are bound by the Act both as employers (how they treat staff) and as service providers (how they treat the people they care for). The protections under the nine protected characteristics apply, the duty to make reasonable adjustments applies, and for public-sector providers the Public Sector Equality Duty applies on top.
Equality and diversity in care are practical, daily concerns rather than abstract policy ideas. They sit on the foundation of the Equality Act 2010, connect to what equality and what diversity mean more broadly, and overlap with cultural diversity in particularly direct ways. To equip your care team to apply these principles confidently in everyday work — meeting Care Certificate Standard 4 and the wider regulatory framework — our Equality, Diversity & Inclusion Training course is built specifically for UK care settings and is current to the recent legal developments.
Related guides
- Equality Act 2010: The Complete UK Guide
- The Nine Protected Characteristics Under the Equality Act 2010
- Neurodiversity at Work: A UK Employer's Guide
Equip your care team to apply equality and diversity confidently in everyday work.
Explore the Equality, Diversity & Inclusion course →
Mark writes about equality, diversity and inclusion, workplace compliance and accredited online training for Equality, Diversity & Inclusion Training, part of Online CPD Academy.